Infection Control & Prevention in Dental Practice
Dr. C. Habib

Objectives
This article is intended to provide readers with information about:
- The infection and control measures applicable to dentistry in the United Kingdom, taking into account current knowledge about infection transmission.
- The need to establish clear policies and procedures to ensure that all employees adhere to the required standards for infection control and prevention.
Introduction & Background
As in all medical practice, it is easier to prevent infection occurring in the first place rather than have to control and treat infection once it has taken hold. While accepting that the risk of infection in dentistry is low, the risks still need to be mitigated against, and infection prevention and control is an important consideration when it comes to patient safety.1
A dental practice needs to integrate effective infection prevention and control measures into an overall risk management program. This will help to ensure the quality of patient care and protect the occupational health of dentistry staff.4
Ethical & Legal Responsibilities
All UK dental practices have an ethical and legal responsibility to effectively control and prevent infections. The General Dental Council states that 'failure to employ adequate methods to prevent cross infection would almost certainly render a dentist liable to a charge of serious misconduct.' 2,4
To ensure that dental practices are aware of the required quality standards and latest best practice, the Department of Health published its Health Technical Memorandum 01-05: Decontamination in primary care dental practices (latest edition 2009). These HTM 01-05 guidelines stipulate the correct procedures to follow and the products that should be used to prevent infection. All dental practices must adhere to these guidelines.3
As well as complying with the HTM 01-05 guidelines, each dental practice must establish its own infection control policy. This policy must address the particular requirements of the practice. It also needs to be a written policy, readily available to all employees and regularly updated.
Employee Training
Employees are more likely to comply with infection prevention and control measures if they understand the rationale for them.1
New employees should be trained in the necessary protocols on joining the practice, before taking on new tasks or procedures, or using new equipment. It's imperative that an employee's training is ongoing and regularly reviewed or updated. Employees also need to be shown how to reduce the risk of being infected themselves and how to effectively manage any work-related illness or injury.1
Standard Principles of Infection Control
As the source of infection cannot always be identified or traced, it is important that the necessary precautions are always taken to prevent infection. Routine procedures have been established that are known as 'Standard Principles of Infection Control' or 'Universal Precautions'.2,4
These principles generally cover the following elements:
- Protective clothing.
- Hand hygiene and skin care.
- Safe handling of sharps.
- Spillage management.
Protective clothing
The standard principles for the use of single use disposable gloves are as follows:
- Gloves must conform to European Community standards (EN 455, parts 1,2,3) and US standards (ASTM 1671-97).
- Disposable gloves may be worn in the following circumstances:
- when there is likely to be contact with sterile sites
- when invasive procedures are required
- when a risk of transmitting infection has been identified.4
- As the name implies, single use gloves can only be used as such, and must be correctly disposed of after use.
There are other considerations that influence glove selection. Generally, the following recommendations are observed:
- Use non-sterile gloves for cases in which contact with bodily fluids (even fluid on equipment) will occur.
- Use sterile gloves for surgical procedures or when there will be contact with sterile areas.
- Use general purpose gloves for cleaning instruments before they are sterilised or when there is likely to be contact with contaminated surfaces.
- Don't use polyurethane or polythene gloves in any circumstances.4
The use of plastic aprons is appropriate for circumstances in which clothing may come into contact with bodily fluid.4,5 Aprons are also items of protective clothing that are designed for single use only.
Protective eyewear should be worn by both the dentist and patient during procedures.1,4 This helps prevent blood or other bodily fluid from getting into the dentist's or patient's eyes. It's essential that eyewear is disinfected after use, and, in the case of patient eyewear, in-between patients.6
Dentists should also wear facemasks for similar reasons to that given for eye protection.
Hand hygiene and skin care
Evidence indicates that approximately 80 per cent of nosocomial infections are passed on by the hands.11 Hand washing is therefore fundamental to the control and prevention of infection. Nowadays, it is more correct to refer to the importance of 'hand hygiene' rather than hand washing, as alcohol-based rubs are used to clean hands as well as liquid soaps.1
Hand hygiene is about more than washing the hands; there are other precautions to take to ensure that hands are sufficiently clean. Any cuts or abrasions should be adequately covered by waterproof dressings. Fingernails should be kept short and clean. Nail polish can harbour germs and should not be worn.4,7,8
Hands must be washed frequently throughout the day, and, in particular, in the following circumstances:
- before and after work or any work breaks
- before and after eating, drinking or handling food
- before and after smoking
- before and after physical contact with patients
- before putting on and after taking off any protective clothing
- after using the toilet
- after blowing nose or covering a sneeze
- after any time that hands are visibly soiled.4
An effective hand hygiene technique consists of the following steps:
- Preparation.
- Washing and rinsing.
- Drying.
In preparation for cleaning hands, remove all hand jewellery. Hands should be wet under tepid running water before soap is applied.4
It is important that the soap covers the entire hand surface while washing and rinsing. Vigorously rub hands for a minimum of 10-15 seconds. Particularly focus on cleaning finger tips, thumbs and the spaces between the fingers.4 Hands should be thoroughly rinsed, with all traces of soap removed.
The 'Anatomic Scrub Technique'8 is an effective method of ensuring that hands are adequately cleaned. This technique is shown in the diagram below.
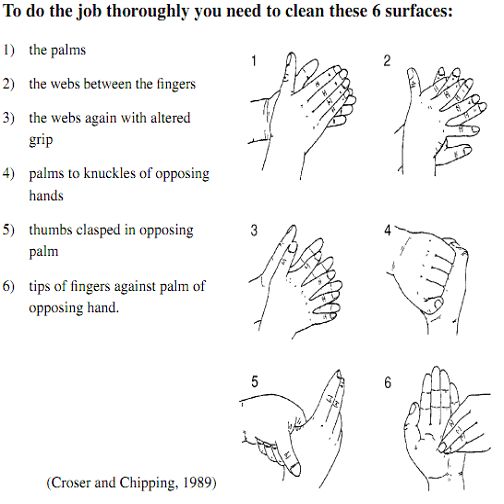
Figure 1 (Source: MacLean C, 2005)
Thoroughly dry hands after washing. Paper towels should be used rather than communal hand towels, which can be a source of cross-contamination.4
Safe Handling of Sharps
If possible, avoid the use of sharp instruments. When sharp instruments are required to be used, they should be used and disposed of safely and carefully. This will reduce the risk of 'needle stick injury' and exposure to blood-borne viruses.4 It is also essential that staff are correctly trained in the use of sharp instruments, and that certain procedures, such as injections, are only carried out by suitably qualified staff.
Spillage management
Because of the infection risks associated with blood and bodily fluid, it is necessary to take precautions to prevent exposure. Wearing protective clothing is one way of reducing the risk. Another essential tool is a blood spillage kit. Such a kit should be readily to hand in case of blood spill, and the kit should be maintained and replenished after use.4
Decontamination in Dental Practice
To prevent cross infection, medical instruments and the environment must be decontaminated using safe, reproducible and scientific methods.3
Decontamination comprises the following stages:
- Cleaning: The physical removal of contamination and micro-organisms using hot water and detergent.4 All 'low-risk' items that have come into contact with intact skin should be cleaned. Mechanical cleaning, using either a washer/disinfector or an ultrasonic bath, is recommended for dental practices.9
- Disinfection: Reducing the number of micro-organisms to a level that is not harmful.10 All 'medium-risk' items that have come into contact with mucous membranes or which may be contaminated should be disinfected. This can be achieved by the application of heat or chemical disinfectants.
- Sterilisation: Sterilisation achieves the removal or destruction of all micro-organisms, and is achieved by applying pressurised steam or dry heat.10 All items that fall into the high risk category of having penetrated skin or mucous membranes, or which have entered sterile body areas, must be sterilised.
The following are guidelines for ensuring that a dental practice is decontaminated:
- Keep the practice clean and free from dirt and dust.
- Establish a cleaning schedule which defines who is responsible for cleaning, how often cleaning should be carried out, how cleaning should be carried out and the expected outcomes.4
- Establish a clean zone and dirty zone. When cleaning, begin in the clean zone and work from the cleanest area to the dirtiest area. This reduces the risk of cross contamination.4
- When not in use, keep mops and buckets clean and dry and store them correctly (mop stored head up, bucket inverted).4
- Decontaminate instruments immediately after use.3 The decontamination method used should be based upon the level of risk associated with the instrument and level of decontamination.4
- Only staff adequately trained in the necessary procedures should carry out the decontamination. Items should be physically cleaned before decontamination.
- Avoid manual cleaning, except after an automated or enzymatic cleaning bath. Change the autoclave reservoir daily.3
- Carry out daily checks of the sterilising machine to ensure that it is working effectively. Do this in accordance with established practice protocol or by using a chemical test strip.3
- Store all instruments in a dry airtight container, in accordance with HTM 01-05 requirements.3
- Keep all instruments that are located within two metres of the dental chair covered to reduce the risk of airborne transmission of infection.3
It is also important to decontaminate areas that patients may come into contact with throughout the day. After each patient has been seen, the single-use protective cover on the hand controls of the chair should be removed. The chair and hand controls should be cleaned before a new cover is placed on the chair. Any surfaces within a two metre radius of the dental chair (the high risk zone) should also be cleaned and disinfected. Once the final patient has been treated all work surfaces and the floor should be cleaned and disinfected.3
Alcohol-based surface cleaners are not recommended for cleaning surfaces in a dental practice. Hot water and detergent should first be used to clean surfaces before wiping surfaces down with a 0.1% (1000 ppm available CI) hypochlorite disinfectant solution.4
Colour Coding System for Hygiene
A colour coding system is designed to prevent cross contamination. It helps to identify areas that are at high risk of cross contamination, and covers the use of cleaning equipment and gloves.4 A colour coding system based on the National Colour Coding System for the British Institute of Cleaning Science is often recommended, and is indicated in Diagram 2 below.
When dealing with disposable items it is essential that the colour coded system is monitored and controlled against new stock release.4
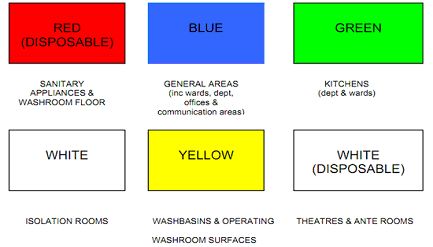
Figure 2 (Source: Department of Health, Social Services and Public Safety, 2011)
Immunisation
Any staff likely to handle sharps or clinical waste should have a complete course of immunisation against Hepatitis B, as well as checks on their antibodies level. Employers need to ensure that new staff or existing staff without sufficient protection have a prompt risk assessment for Hepatitis B vaccination.4
Conclusion
Infection prevention and control forms an important part of practice for all health care professions including dentistry. In dental practice, both patients and health care workers may be exposed to a number of blood borne and upper respiratory pathogens. Professional dental associations, including provincial licensing authorities in the United Kingdom, have advocated that universal precautions be applied to all patients, as their potential infectivity may not be known. Dental offices and the staff should also utilise the full range of recommended infection control procedures that are necessary to minimise the risk of cross-infection in dental practice.
|
Safety Priorities highlight safety issues in the dental surgery - click here to watch a comical short film



|


